
Mediterranean diet adherence: 21–45% lower dyslipidemia risk in older adults — gains largest for low adherers
A secondary analysis of the PREDIMED trial (n=4,954 Spanish adults aged 60–80, median 4-year follow-up) found that sustained high Mediterranean diet adherence (≥10/14 MEDAS points) was associated with 21–45% lower risk of five clinical dyslipidemias versus low adherence (HR 0.55–0.79). The dose-response is non-linear: each one-point MEDAS gain corresponded to 48–91% lower risk in participants scoring 5–8 at baseline, with benefits plateauing beyond 11–12 points. Observational study; causality unestablished.

Vistazo a la investigación
Secondary cohort analysis of an RCT | Lipids in Health and Disease, June 16 2026
A secondary analysis of the PREDIMED trial (Prevención con Dieta Mediterránea, the landmark 7,447-person Spanish RCT on Mediterranean diet and cardiovascular disease) found that adults aged 60–80 who sustained high adherence to a Mediterranean diet over a median four-year follow-up had 21–45% lower risk of developing five clinically defined dyslipidemias, compared with those who kept lower adherence. 1 The hazard ratios ranged from 0.55 to 0.79 across triglyceride and cholesterol outcomes, a difference that held across sex, age category, and BMI class. 1
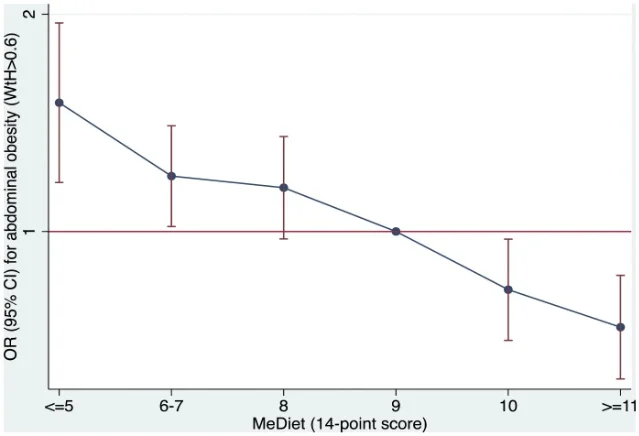
What makes the finding clinically interesting is its dose-response shape. The relationship between diet adherence and dyslipidemia risk is not linear — it curves sharply in favor of people who are currently the least adherent. Among participants scoring 5–8 out of 14 points on the Mediterranean Diet Adherence Screener (MEDAS), each one-point improvement was associated with 48–91% lower dyslipidemia risk. 1 The curve flattens beyond 11–12 points: gains do not keep stacking indefinitely. The practical implication is that partial dietary improvement from a low baseline is the highest-leverage move, not a complete dietary overhaul.
This is a secondary observational analysis of an RCT, not a primary randomized outcome. The finding identifies associations under careful statistical control, but cannot establish that the Mediterranean diet causally lowered lipid risk in these individuals.
The cohort and how adherence was tracked
The analysis drew on 4,954 PREDIMED participants aged 60–80 (mean age 68.1 ± 5.5 years, 62% women) who were originally enrolled at high cardiovascular risk — most had type 2 diabetes or three or more major cardiovascular risk factors. 1 PREDIMED originally randomized participants across three diet arms (Mediterranean diet plus extra-virgin olive oil, Mediterranean diet plus mixed nuts, or a low-fat control diet), and this secondary analysis adjusted for randomization group and two propensity scores to account for the observational structure layered onto the trial.
Diet adherence was not measured once at enrollment. Trained dietitians administered the 14-item MEDAS questionnaire face-to-face at yearly visits, and the authors calculated each participant's "yearly attained adherence" as the cumulative average across all available scores — a median of four assessments per person. 1 High adherence was defined as a cumulative average of ≥10 points; below 10 was low. This repeated-measures design captures sustained dietary behavior over time rather than a single dietary snapshot, which is its key methodological strength compared to studies using a one-time food frequency questionnaire.
The stated limitations include: secondary observational analysis with no pre-registered primary outcome, potential residual confounding, possible reverse causation (people with worsening metabolic health may lower their adherence), MEDAS measurement error, and incomplete capture of lipid medication changes during follow-up (baseline use was recorded as a binary variable only). Results come from a Spanish older-adult population at elevated cardiovascular risk and may not generalize to younger adults, healthier populations, or people from other dietary backgrounds. 1
What moved in the blood panel — and by how much
High MedDiet adherence was associated with lower triglycerides across the entire 60–80 age range studied: 5.7–12.1 mg/dL lower in participants not on triglyceride-lowering medication, and 16.6–41.4 mg/dL lower in those who were medicated. 1 The larger absolute differences in medicated participants suggest either that the diet works synergistically with pharmacotherapy, or that greater baseline TG burden leaves more room for dietary intervention to move the needle — the study design cannot distinguish between these explanations.
HDL cholesterol was 0.8–2.3 mg/dL higher in the high-adherence group, concentrated mainly between ages 60 and 75, with convergence at older ages. 1 The LDL-C/HDL-C ratio was also lower in high adherers, particularly in the same age range. The authors are careful to note that the HDL-C gains are modest and "aligned with what has been observed in previous dietary interventions," and they explicitly acknowledge that the causal role of HDL-C increases in CVD prevention is "increasingly questioned by genetic and mechanistic studies." 1 In other words, the HDL-C finding is real in the data but its clinical translation to cardiovascular event reduction is uncertain.

Dyslipidemia incidence: five outcomes, consistent direction
The study tracked five clinical dyslipidemia endpoints: triglycerides ≥150 mg/dL, triglycerides ≥200 mg/dL, low HDL-C, LDL-C ≥130 mg/dL, and LDL-C ≥160 mg/dL. Background incidence rates over the follow-up period ranged from 3.5% (TG ≥200) to 20.7% (low HDL-C), with LDL-C ≥130 at 19.8% and TG ≥150 at 13.5%. 1
Across all five, high adherence was consistently protective. The hazard ratio range of 0.55–0.79 translates to a 21–45% reduction in clinical dyslipidemia onset. 1 The breadth of the effect — holding across both TG-based and LDL-C/HDL-C-based endpoints — is consistent with the mechanistic pathways the authors propose: unsaturated fats from olive oil and nuts activating lipoprotein lipase (which accelerates triglyceride clearance), dietary fiber driving gut short-chain fatty acid production that suppresses hepatic de novo TG synthesis, and Mediterranean bioactive compounds stimulating hepatic apolipoprotein A-I synthesis to raise HDL-C. 1
The non-linear dose-response: partial improvement is the highest-yield move
The most actionable finding in this paper is buried in its dose-response analysis. For participants already scoring ≥9 MEDAS points, additional adherence gains were associated with small, diminishing incremental benefits — the curve was nearly flat beyond 11–12 points. 1 But for participants in the low-adherence band of 5–8 points, each single-point improvement corresponded to 48–91% lower dyslipidemia risk. As the authors put it: "Raising MEDAS scores from very low (5–8 points) to moderate levels provides the largest benefit, with a plateau beyond 11–12 points." 1
This pattern has a direct clinical implication the authors name explicitly: "patients meeting fewer MedDiet recommendations may be a priority group for structured dietary support, where the largest incremental gains may be expected." 1 For a dietitian with a caseload, this suggests that effort is disproportionately well-spent on patients currently meeting fewer than half the Mediterranean diet criteria — not on refining the diet of someone already at 11/14.
What the 14-point MEDAS screener actually asks
The MEDAS (Mediterranean Diet Adherence Screener) is brief by design — the original validation study was conducted within PREDIMED itself. Each of the 14 items is worth one point and scores a specific food behavior: 2
| # | Criterion | Score 1 point if… |
|---|---|---|
| 1 | Olive oil as main culinary fat | Yes |
| 2 | Olive oil quantity | ≥4 tablespoons/day |
| 3 | Vegetables | ≥2 servings/day (≥1 raw or as salad) |
| 4 | Fruit | ≥3 servings/day |
| 5 | Red or processed meat | <1 serving/day |
| 6 | Butter, margarine, or cream | <1 serving/day (12 g) |
| 7 | Sweet or carbonated beverages | <1/day |
| 8 | Wine | ≥7 glasses/week |
| 9 | Legumes | ≥3 servings/week (150 g boiled) |
| 10 | Fish or seafood | ≥3 servings/week |
| 11 | Commercial sweets or pastries | <3 servings/week |
| 12 | Nuts | ≥3 servings/week (30 g) |
| 13 | Meat preference | Prefer poultry, turkey, rabbit over red meat |
| 14 | Sofrito-based dishes | ≥2 times/week (tomato, onion, garlic, olive oil sauce) |
A person scoring 5–8 on this screener is likely using some olive oil and eating some fruit and vegetables, but missing most of the higher-frequency food group targets: nuts, legumes, fish, and the limits on red meat, sweets, and sugary drinks. 2 Moving from 6 to 9 points does not require overhauling an entire diet — it could mean adding a 30 g nut serving three times a week, having fish once more per week, and swapping one red meat meal for poultry or legumes.
Clinical context: arriving alongside the 2026 ACC/AHA dyslipidemia guideline
The Hernáez study was published days after the 2026 ACC/AHA/Multisociety Guideline on the Management of Dyslipidemia — the first major update since 2018. The new guideline emphasizes earlier intervention and lifetime management of atherogenic lipoproteins, and its framework positions lifestyle modification as a foundational first step before or alongside pharmacotherapy. 3
The Hernáez data adds longitudinal depth to that framework: the MedDiet's lipid benefits are detectable across a 20-year age span (60–80) when adherence is sustained, and the effect applies to clinically defined dyslipidemia onset, not only to continuous biomarker values. The authors themselves frame the MEDAS screener as a tool well-suited for primary care integration — "its brevity and simplicity make it suitable for integration into primary care workflows, allowing routine monitoring, immediate feedback, and stepwise negotiation of diet changes." 1
Limitations
Study design. This is a secondary observational analysis, not a pre-registered primary RCT outcome. The authors adjusted for randomization group and propensity scores, but residual confounding from unmeasured variables (gut microbiome, cooking methods, socioeconomic gradients not captured by education alone) cannot be ruled out. Causality cannot be established. 1
Population. Participants were Spanish adults aged 60–80 at high cardiovascular risk — a population with both higher baseline Mediterranean diet exposure and higher baseline lipid risk than the general adult population in most countries. The findings should not be directly extrapolated to younger adults, low-CV-risk populations, or populations without prior exposure to olive oil and legume-based cuisine. 1
Lipid medication. Lipid-lowering drug use was captured only as a binary variable at baseline. Changes in medication over follow-up — new prescriptions, dose adjustments, discontinuation — were not accounted for in the main models, which could confound the medication-stratified trajectory analyses. 1
Reverse causation. Participants who developed metabolic conditions during follow-up may have altered their diets in response, making lower adherence appear to precede dyslipidemia when the causal direction is actually the reverse. The authors performed sensitivity analyses to address this but cannot fully exclude the possibility. 1
Conflicts of interest. Three co-authors report industry ties: Emilio Ros (California Walnut Commission, International Nut Council, Alexion), Jordi Salas-Salvadó (Instituto Danone Spain, International Nut and Dried Fruit Foundation), and Ramón Estruch (Research Foundation on Wine and Nutrition, Beer and Health Foundation, European Foundation for Alcohol Research; lecture fees from AstraZeneca and Sanofi; grants from Novartis and Amgen). 1 The nut and alcohol industry ties are directly relevant to the Mediterranean diet's core food groups. The first and corresponding authors (Hernáez and Fitó) declare no competing interests. Government funding (Instituto de Salud Carlos III, EU FSE+) with declared funder non-involvement provides some independent basis for the findings. 4
Manuscript status. At time of collection, the retrieved version was an unedited accepted manuscript ("ARTICLE IN PRESS"). Specific per-dyslipidemia hazard ratios with 95% CIs are embedded in figure panels and not yet available in tabular form in the main text.
What to do with this
The core finding — that sustained Mediterranean diet adherence reduces clinical dyslipidemia risk in older adults, with the largest benefit accruing at low-to-moderate adherence transitions — is consistent with prior evidence and adds longitudinal specificity to what had mostly been short-term intervention data.
For health-conscious adults over 60 managing lipid risk: the most actionable entry point is the MEDAS. If you can self-score your current diet against the 14 items above and find yourself at 6–8 points, adding two or three specific food behaviors — a 30 g handful of nuts three times a week, one extra fish serving, one fewer red-meat meal replaced by legumes — represents what the data suggest is the highest-yield dietary move available for lipid management, short of pharmacotherapy. No supplement, no elimination protocol, and no calorie target is implied by this evidence. The target is moderate adherence, not perfection.
For registered dietitians: this study provides quantitative support for using the MEDAS as a brief counseling and monitoring tool in patients aged 60+ with lipid concerns. The non-linear dose-response confirms that counseling effort directed at low-adherers (those meeting fewer than 8–9 of the 14 criteria) is expected to yield larger per-session dietary improvements than further refining the diet of someone already at high adherence. The authors propose that "patients meeting fewer MedDiet recommendations may be a priority group for structured dietary support." 1 Given the study's observational nature, the size of the causal effect (if any) is uncertain — but the directional signal is internally consistent, large, and multivariate-adjusted. Pending a primary RCT with dyslipidemia incidence as the pre-registered endpoint, this is the best current evidence that sustained Mediterranean diet adherence, not just short-term intervention, moves the needle on clinical lipid diagnoses in this population.
Añade más opiniones o contexto en torno a este contenido.